The air at 5,000 metres contains exactly the same proportion of oxygen as the air at sea level , 20.9 percent. This fact surprises most people. They assume high altitude means less oxygen. It does not. What it means is less air pressure pushing that oxygen into your lungs, and from your lungs into your blood, and from your blood into your muscles and brain. The result is the same , your body receives less oxygen , but the mechanism matters because it explains why acclimatisation works and why no amount of fitness can substitute for it.
At sea level, the atmospheric pressure is roughly 1,013 millibars. At the summit of Kala Patthar , 5,545 metres, the highest point on the standard Everest Base Camp trek , the pressure drops to approximately 505 millibars. Half. Your lungs, evolved over millions of years to operate at sea-level pressure, suddenly have to extract the same oxygen from air that is pushing half as hard. The oxygen is there. It simply will not come in as easily.
Your body can adapt to this. It has done so for millennia , populations in Tibet, the Andes, and the Ethiopian highlands have lived above 3,000 metres for thousands of years. But adaptation takes time. Weeks for the initial response. Months for full adjustment. The trekker who flies from London to Lukla and starts walking uphill has neither weeks nor months. They have days. And in those days, their body must accomplish a series of physiological changes that determine whether the trek ends in triumph or in a helicopter.
What happens to your body at high altitude?
The first thing that happens , within hours of arriving above 2,500 metres , is that your breathing rate increases. Your body detects the lower oxygen saturation in your blood and tells your lungs to work harder. You breathe faster. You breathe deeper. This is not a sign of unfitness. It is a sign that your body is doing exactly what it should.
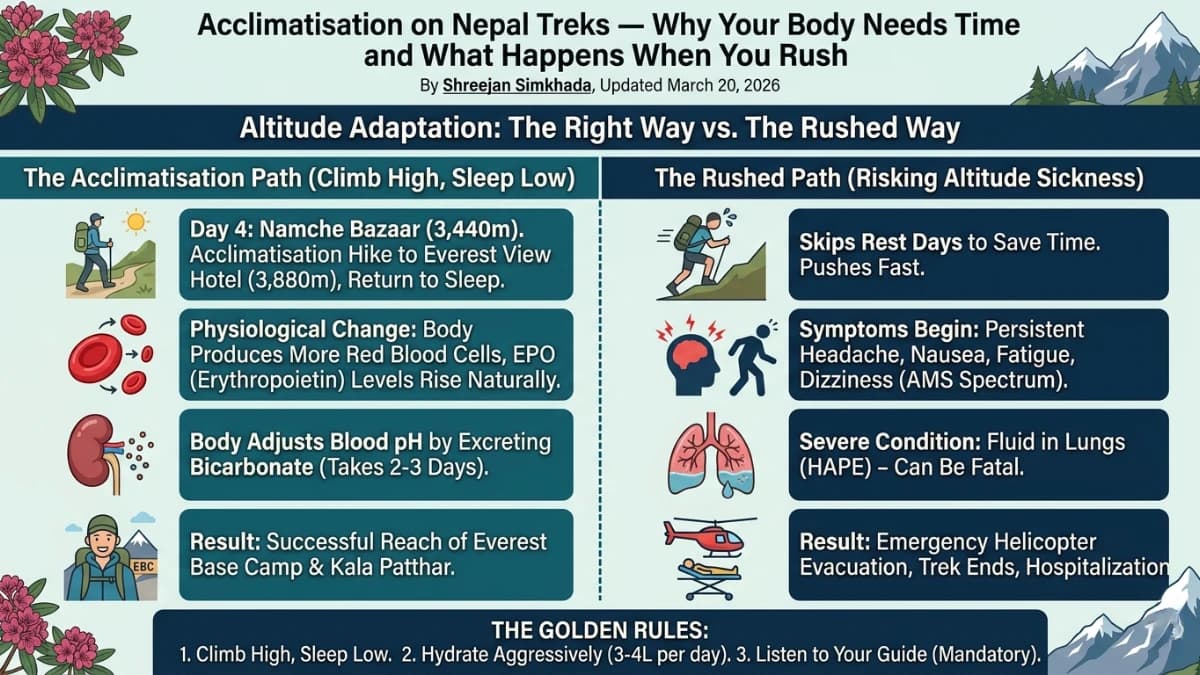
Over the next two to three days, your kidneys begin excreting bicarbonate , a base that normally buffers the acidity of your blood. With less bicarbonate, your blood becomes slightly more acidic, which shifts the oxygen-haemoglobin dissociation curve in a direction that helps oxygen release from your blood into your tissues. This is chemistry that no amount of training can accelerate. It takes the time it takes.
Your heart rate increases. Your body produces more red blood cells , a process triggered by erythropoietin (EPO), the same hormone that disgraced cyclists inject. At altitude, your body manufactures it naturally and legally. More red blood cells mean more haemoglobin, which means more oxygen-carrying capacity. This process begins within days but takes weeks to reach its full effect.
Your blood vessels in the lungs constrict in response to low oxygen , a process called hypoxic pulmonary vasoconstriction. This is supposed to redirect blood toward better-ventilated areas of the lung. But if the constriction is too aggressive or too widespread, it raises the pressure in the pulmonary arteries and can lead to fluid leaking into the lungs. This is the beginning of High Altitude Pulmonary Edema , HAPE , one of the two potentially fatal altitude illnesses.
Your brain, meanwhile, is dealing with its own crisis. The blood-brain barrier , the membrane that controls what enters your brain from your bloodstream , becomes more permeable at altitude. Fluid leaks into the brain tissue. A small amount of swelling is normal and causes the mild headache that most trekkers experience above 3,500 metres. An excessive amount of swelling is High Altitude Cerebral Edema , HACE , which is rarer than HAPE but more rapidly fatal.
All of these processes are happening simultaneously inside your body as you walk through the most beautiful mountains on earth. You do not feel most of them. What you feel is the headache, the breathlessness, the loss of appetite, the difficulty sleeping. These are the symptoms of your body working to adapt. They are normal. They are expected. They pass , if you give them time.
What does climb high sleep low mean for trekkers?
Three words that have saved more lives in the mountains than any piece of equipment: climb high, sleep low. The principle is simple. During the day, you walk to a higher altitude, exposing your body to the reduced pressure and triggering the adaptive responses. At night, you descend to a lower altitude to sleep, giving your body time to process the changes in thicker air.
On the Everest Base Camp trek, this principle is built into every well-designed itinerary. The acclimatisation day in Namche Bazaar (3,440 metres) is the most important day of the trek , not because of what you see, but because of what your kidneys, lungs, and blood are doing while you hike up to the Everest View Hotel at 3,880 metres and then walk back down to sleep at 3,440. You climbed high. You slept low. Your body used those hours to adapt.
The second acclimatisation day in Dingboche (4,410 metres) repeats the pattern at a higher altitude. You hike up toward 5,000 metres , perhaps to the Nangkartshang viewpoint , and return to Dingboche to sleep. Two acclimatisation days. Two critical opportunities for your body to adjust. Skip either one and the risk of serious altitude sickness increases dramatically.
Some trekkers , particularly fit ones , chafe at rest days. They feel fine. Their legs are strong. The trail is calling. They want to push ahead. This is precisely when the most dangerous decisions are made, because the symptoms of altitude sickness are delayed. You feel the effects of yesterday's altitude today. The headache that arrives at Lobuche was triggered by the gain from Dingboche the day before. By the time you feel bad, the damage is already in progress.
What are the symptoms and stages of altitude sickness?
Acute Mountain Sickness , AMS , is not a binary condition. It is a spectrum. Almost every trekker who sleeps above 3,500 metres experiences some symptoms. The question is not whether you will feel the altitude but how severely and how your body responds to the rest and hydration that constitute the first line of treatment.
Mild AMS , headache, loss of appetite, nausea, difficulty sleeping, fatigue, dizziness. These symptoms affect the majority of trekkers above Namche. They are uncomfortable but not dangerous. Treatment: rest, hydration (three to four litres per day), paracetamol for headache, and , critically , do not ascend further until symptoms resolve. Most mild AMS resolves within twenty-four to forty-eight hours.
Moderate AMS , persistent headache not relieved by paracetamol, vomiting, marked fatigue, shortness of breath at rest, difficulty walking in a straight line. This is the body sending a clear message: something is going wrong. Treatment: do not ascend. If symptoms do not improve with rest, descend at least 500 metres. Acetazolamide (Diamox) can accelerate acclimatisation but does not treat the underlying problem , only descent does.
Severe AMS / HACE , confusion, inability to walk in a straight line (ataxia), altered consciousness, hallucinations, extreme fatigue, aggression or withdrawal. This is a medical emergency. Descend immediately , by any means available, including helicopter if necessary. Dexamethasone can buy time but is not a substitute for descent. HACE kills people who stay at altitude. It does not kill people who descend.
HAPE , persistent cough (often productive with pink or frothy sputum), extreme breathlessness at rest, chest tightness, gurgling sounds when breathing, blue lips or fingertips. HAPE can develop independently of AMS or alongside it. It is more common than HACE and equally deadly if untreated. Treatment: immediate descent, supplemental oxygen if available, nifedipine as a temporising measure. Like HACE, HAPE resolves with descent. Like HACE, it kills at altitude.
Do I need a guide to manage altitude on Nepal treks?
A trained trekking guide carries a pulse oximeter , a small device that clips onto your finger and measures the oxygen saturation of your blood. At sea level, your SpO2 is typically 95-100 percent. At Namche, a reading of 85-90 percent is normal. At Gorak Shep, 75-85 percent is expected. Your guide checks these numbers every morning and every evening.
The numbers alone do not determine the decision to continue or descend. A trekker with an SpO2 of 78 percent who feels well, is eating normally, and is sleeping (even poorly) is acclimatising. A trekker with an SpO2 of 82 percent who has a persistent headache, is not eating, and is stumbling on the trail may be in trouble despite the "better" number. Your guide reads the numbers in context , combining the oximeter data with visual observation, conversation, and years of experience watching bodies adapt and fail at altitude.
This is why the mandatory guide rule in Nepal, for all the controversy it generated, makes medical sense. A solo trekker with AMS symptoms faces a dangerous decision-making problem: the organ they need to make good decisions , their brain , is the organ being affected by the altitude. Confusion, poor judgment, and stubbornness are symptoms of altitude sickness. The person least qualified to decide whether to descend is the person who needs to descend. A guide provides the external judgment that the trekker's impaired brain cannot.
Should I take Diamox for altitude sickness on Nepal treks?
Acetazolamide , sold as Diamox , is a carbonic anhydrase inhibitor originally developed for glaucoma. Its effect on altitude acclimatisation was discovered almost by accident: patients taking Diamox for their eyes reported feeling better at altitude. The mechanism is elegant. Diamox forces your kidneys to excrete bicarbonate faster, which accelerates the blood pH shift that normally takes days. It essentially speeds up one of the key acclimatisation processes.
Diamox is not a magic pill. It does not prevent altitude sickness. It accelerates acclimatisation, which reduces the risk. The difference matters. A trekker on Diamox who ascends too fast will still get sick. A trekker on Diamox who follows a proper acclimatisation schedule will acclimatise faster and more comfortably than they would without it.
The standard prophylactic dose is 125mg twice daily, starting one to two days before ascending above 3,000 metres. Common side effects: tingling in the fingers and toes (almost universal), increased urination (the drug is a diuretic), altered taste (carbonated drinks taste flat and metallic), and , rarely , nausea and fatigue.
The tingling is harmless but disconcerting if unexpected. The increased urination means more water intake is essential , dehydration at altitude compounds altitude sickness. The altered taste is temporary and resolves when the drug is stopped.
Should you take it? This is a conversation for your doctor, not your trekking company. Many experienced trekkers use it. Many do not. Some take it as a prophylactic. Some carry it as a treatment to start only if symptoms appear. There is no single right answer. But there is a wrong answer: taking Diamox and using the perceived protection as justification to skip acclimatisation days or ascend faster than the itinerary allows.
How much water should I drink at altitude on treks?
Your body loses water at altitude at a rate that would alarm you if you measured it. The air is dry , humidity at 5,000 metres is typically below 20 percent, compared to 40-60 percent at sea level. Every breath you exhale carries moisture that is not replaced by the dry air you inhale. You breathe faster at altitude. You lose more water per hour. The cold suppresses your thirst reflex , you do not feel thirsty even as you dehydrate.
Three to four litres of water per day is the minimum recommendation above 3,000 metres. This sounds like a lot. It is a lot. And it needs to be consumed steadily throughout the day, not in large gulps at mealtimes. A water bottle in the side pocket of your daypack, sipped every fifteen to twenty minutes, is the most effective delivery system.
The colour of your urine is the simplest hydration indicator. Clear or pale yellow means adequate hydration. Dark yellow means you are behind. By the time you are producing dark urine at altitude, you are significantly dehydrated, and dehydration mimics and worsens the symptoms of AMS.
Hot drinks count toward your fluid intake. Tea at every stop. Soup with every meal. Hot lemon and honey , a Himalayan trail staple , provides hydration, warmth, and a psychological boost that should not be dismissed. The ritual of stopping at a teahouse, wrapping cold hands around a metal cup of sweet tea, and sitting quietly for twenty minutes is not laziness. It is acclimatisation strategy disguised as comfort.
Why is it hard to sleep at high altitude?
You will not sleep well above 4,000 metres. This is normal. It is not a sign of illness. It is a direct consequence of the same respiratory changes that are helping you acclimatise.
At altitude, your breathing pattern changes during sleep. Your body alternates between periods of deep breathing and periods of very shallow breathing or no breathing at all , a pattern called Cheyne-Stokes respiration or periodic breathing. You breathe deeply for several cycles, then your breathing slows, pauses, and you wake up with a gasp. This happens dozens of times per night. It is frightening the first time. It is annoying every time after.
Periodic breathing is caused by the conflict between two respiratory drives. Your oxygen sensors say breathe more. Your CO2 sensors , which have been recalibrated by the bicarbonate excretion , say breathe less. During waking hours, conscious breathing overrides the conflict. During sleep, the automatic system oscillates between the two signals.
Diamox reduces periodic breathing , it is one of the drug's most appreciated benefits. Sleeping with your head elevated also helps. Some trekkers find that sleeping on their side rather than their back reduces the severity. Nobody finds a complete solution. The thin mattresses, cold rooms, and coughing from nearby bunks do not help.
The best advice is to accept it. You will not get eight hours of deep sleep at Gorak Shep. You will get fragments of sleep interrupted by gasping awakenings, punctuated by trips to the toilet (hydration and Diamox conspire to wake your bladder), and accompanied by the sound of other trekkers experiencing exactly the same thing. And in the morning, you will get up, put on your boots, and walk , because the mountain does not care how well you slept.
Does being fit protect you from altitude sickness?
The single most dangerous misconception about altitude sickness is that fit people are immune. They are not. Research consistently shows no correlation between physical fitness and susceptibility to AMS. Marathon runners get altitude sickness. Olympic athletes get altitude sickness. People who can barely walk a mile at sea level sometimes acclimatise beautifully.
Genetic factors play a significant role. People whose ancestors lived at altitude tend to acclimatise more effectively , but this is population-level genetics, not something an individual can predict. Previous performance at altitude is the best predictor of future performance , if you acclimatised well on a previous trek, you are likely to acclimatise well again. But "likely" is not "certain," and each altitude exposure is its own event.
Age is weakly protective , older trekkers tend to get less AMS than younger ones, possibly because they ascend more cautiously. Gender shows no consistent difference. Body weight shows no consistent difference. Smoking shows no consistent difference (though it affects endurance, which is a separate issue).
The factor that most reliably predicts altitude sickness is ascent rate. How fast you go up determines, more than anything else, whether your body can keep pace with the demands you are placing on it. This is why itinerary design is not a marketing exercise. It is a medical prescription. The difference between a twelve-day EBC itinerary with two acclimatisation days and an eight-day "fast trek" is not four days of convenience. It is the difference between safe acclimatisation and gambling with cerebral oedema.
How many acclimatisation days does the Everest Base Camp trek have?
Day 4 in Namche Bazaar. You have walked from Lukla or from the road at Phakding, gaining roughly 800 metres of altitude over two days. Your body is just beginning to respond to the reduced oxygen. The acclimatisation hike takes you up to the Everest View Hotel at 3,880 metres , 440 metres above your sleeping altitude , and back down. Total walking time: three to four hours. The views of Everest, Lhotse, and Ama Dablam from the trail above Namche are spectacular. But the views are not the point. The point is the 440 metres of altitude exposure that your body processes overnight while you sleep back at 3,440.
Day 7 in Dingboche. You have now been above 3,000 metres for four days. Your body is adapting but not adapted. The hike above Dingboche takes you to approximately 5,000 metres , the altitude of Everest Base Camp , and brings you back to 4,410. This is a dress rehearsal. Your body experiences the altitude it will face in two days' time and begins preparing. The headache you may have had yesterday is gone. Your appetite returns. Your breathing, which was laboured on the climb to Dingboche, feels almost normal. This is acclimatisation working. This is your body solving the problem of thin air.
These days feel like lost time to ambitious trekkers. They are the opposite. They are bought time , time in which your body makes the changes that will allow you to stand at 5,364 metres at Base Camp and 5,545 metres at Kala Patthar and feel not just alive but exhilarated. The summit day is earned on the rest days. The view from Kala Patthar is paid for in patience at Namche and Dingboche.
What should you do if altitude sickness symptoms appear?
Tell your guide immediately. This is rule number one. Do not minimise symptoms. Do not hide them because you are embarrassed or because you do not want to slow the group. Altitude sickness does not care about your schedule, your deposit, or your pride. It cares about physics and physiology, and it escalates when ignored.
Your guide will assess the situation. Mild symptoms , headache, mild nausea, fatigue , are managed with rest, fluids, and paracetamol. The guide will increase the frequency of oximeter checks. If the itinerary allows, you may take an extra rest day. If symptoms are moderate , persistent headache, vomiting, significant fatigue , the decision to descend will be made for you, not by you. This is not optional. This is not a discussion. Descent is the treatment. Everything else is temporary.
How far to descend? At least 500 metres, or until symptoms improve. On the EBC route, this is straightforward , the trail goes up and down, and lower villages are always accessible. Pheriche has a medical clinic (the Himalayan Rescue Association post, staffed by volunteer doctors during trekking season) that provides altitude sickness assessment and treatment. Namche Bazaar has additional medical facilities. Lukla has an airstrip for evacuation to Kathmandu.
Helicopter evacuation is available for serious cases. Your travel insurance , which is mandatory and must cover helicopter evacuation to 6,000 metres , pays for this. The helicopter can be called by satellite phone or radio from any point on the trail. Response time depends on weather but is typically within hours during the trekking season. The helicopter flies you to Kathmandu, where hospitals with altitude medicine expertise provide definitive treatment.
The point of all this infrastructure , the guides, the oximeters, the clinics, the helicopters , is not to enable recklessness. It is to provide a safety net for the minority of trekkers whose bodies, despite proper acclimatisation, react adversely to altitude. The net exists. But the best outcome is never needing it. And the best way to never need it is to acclimatise properly, hydrate aggressively, and listen to your body with the same attention you give to the mountains around it.
The Paradox of Altitude
Here is the strange truth about acclimatisation: the process that makes the trek difficult is the same process that makes the summit meaningful. If your body adapted instantly , if you could fly to 5,500 metres and feel normal , the achievement of reaching Kala Patthar would be diminished. It is the difficulty that creates the value. The headache at Namche. The breathlessness at Dingboche. The sleepless night at Lobuche. The slow, deliberate, one-foot-in-front-of-the-other walk across the Khumbu Glacier to Base Camp. Each of these experiences is your body fighting to give you something extraordinary, and the fight is what makes the gift worth receiving.
When you stand at the summit of Kala Patthar at dawn and watch the first light touch the summit of Everest, you will be breathing hard. Your oxygen saturation will be in the high seventies. Your heart will be working fifty percent harder than it does at sea level. Every system in your body will be operating at the edge of its capacity. And you will feel , not in spite of this but because of it , more alive than you have ever felt at a desk, in a car, or in any comfortable room at sea level.
That feeling is acclimatisation's final gift. Not the absence of difficulty, but the presence of everything your body has done to bring you here. The red blood cells it manufactured. The breathing patterns it adjusted. The chemistry it recalibrated. All of it , invisible, involuntary, extraordinary , working to keep you alive and upright on a frozen ridge above five thousand metres, watching the sun rise over the highest mountain on earth.
Give your body the time it needs. Follow the itinerary. Drink the water. Take the rest days. And trust that the same biology that makes altitude dangerous also makes altitude conquerable , slowly, carefully, one acclimatisation day at a time.