The sound arrives before the machine. A low, rhythmic thumping that bounces off valley walls and grows louder with each beat until the helicopter materialises from behind a ridge — small, red and white, rotors chopping through air so thin that the pilot is operating at the edge of what physics allows. It descends onto a flat patch of ground near the teahouse, stones and prayer flags scattering in the downdraft, and the door opens.
This happens several times a week during peak trekking season in the Everest and Annapurna regions. A trekker with severe altitude sickness, a broken ankle on loose moraine, a stomach illness that has become dehydration at four thousand metres — the reasons vary but the mechanism is the same. A guide makes the call. A helicopter flies in. A person who was in serious trouble an hour ago is in a Kathmandu hospital bed by afternoon.
The system works. It has saved thousands of lives over the decades. But it is not simple, not cheap, and not without controversy — because where there is money and vulnerability, there are also people willing to exploit both.

How Does Helicopter Evacuation Actually Work in Nepal?
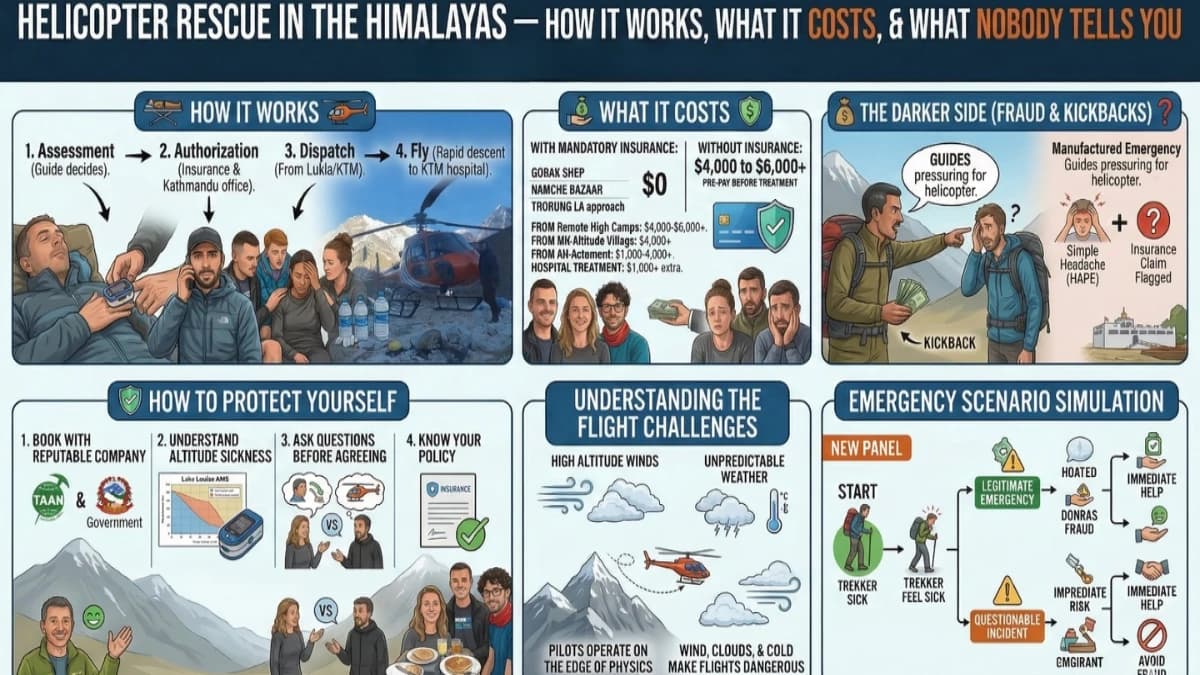
The chain of events begins with your guide. Above 3,500 metres, experienced guides monitor their clients daily — checking pulse oximetre readings each morning, watching for changes in gait, speech, appetite, and alertness. Altitude sickness does not always announce itself dramatically. Sometimes it creeps — a persistent headache that will not respond to ibuprofen, a cough that was not there yesterday, a confusion about simple questions that the trekker does not notice but the guide does.
When the guide determines that a situation requires evacuation, because symptoms are worsening despite descent, because the terrain does not allow rapid descent on foot, or because the patient cannot walk, they contact the company office in Kathmandu. In areas with mobile coverage, this is a phone call. In areas without signal, it is a satellite phone or a message relayed through the nearest teahouse with communication equipment.
The Kathmandu office contacts the helicopter company and the trekker's insurance provider simultaneously. The insurance provider authorises the evacuation, a process that in most cases takes thirty minutes to two hours, though in genuine emergencies it can be expedited to minutes. Once authorised, a helicopter is dispatched from Kathmandu or from a regional base such as Lukla.
Flight time from Kathmandu to the Everest region is approximately forty-five minutes. From Lukla, much less. But weather dictates everything. If cloud fills the valley, if wind exceeds safe parametres, if visibility drops below the pilot's minimum, the helicopter cannot fly. In these cases, and they are not rare, the guide manages the patient's condition on the ground using emergency medication and basic medical care until the weather clears.
The helicopter lands, the patient boards, and the flight to Kathmandu begins. The patient is delivered directly to a hospital, typically CIWEC or Norvic, which have experience treating altitude-related conditions. Treatment begins immediately.
The entire sequence, from the guide's decision to the hospital bed, takes between one and four hours in good weather. In poor weather, it can take a day or more.
How Much Does a Helicopter Rescue Cost in Nepal?
A helicopter evacuation from the Everest region to Kathmandu costs three thousand to six thousand US dollars depending on the pickup location, the number of passengers, and the specific helicopter chartered. Evacuations from higher, more remote locations cost more because the flight is longer and the risk to the pilot greater.
From Gorak Shep or Everest Base Camp: four thousand to six thousand dollars. From Lobuche or Dingboche: three thousand to five thousand. From Namche Bazaar: two thousand to four thousand. From the Annapurna region, similar ranges apply, the Thorong La approach is among the more expensive evacuations due to the altitude and remoteness.
Hospital treatment in Kathmandu adds one thousand to three thousand dollars depending on the condition and the length of stay. Altitude sickness that resolves quickly with descent and supplemental oxygen may require only a day of observation. Severe HAPE or HACE, fluid in the lungs or swelling of the brain, can require several days of intensive care.
With insurance: your cost is zero. The insurance company pays the helicopter operator and the hospital directly. You sign the claim forms. They handle the rest.
Without insurance: you pay the full amount before treatment begins. In cash. At five thousand metres, with your head pounding and your lungs struggling, you negotiate a wire transfer with your family while a helicopter idles on the ground burning fuel at several hundred dollars per hour.
This is why insurance is mandatory. Not recommended. Not suggested. Mandatory.
The Controversy Nobody Wants to Talk About
There is a darker side to helicopter rescue in Nepal that any honest guide must acknowledge. In recent years, reports have surfaced of fraudulent or unnecessary evacuations, situations where trekkers with mild symptoms were pressured by guides or teahouse staff into accepting helicopter evacuation they did not need, because the referring party received a commission from the helicopter company.
The mechanics are straightforward. A guide tells a trekker with a moderate headache that they need immediate helicopter evacuation. The trekker, frightened and disoriented at altitude, agrees. The helicopter arrives. The trekker is flown to Kathmandu. The insurance company is billed four thousand dollars. The guide or the referring party receives a kickback, sometimes hundreds of dollars, sometimes more.
This is not the norm. The vast majority of helicopter evacuations in Nepal are legitimate, necessary, and life-saving. But the fraud exists, and denying it does no service to trekkers who deserve honest information.
How Can You Protect Yourself From Helicopter Scams?
Book with a reputable, TAAN-certified company that pays its guides proper salaries. Guides who earn fair wages have no financial incentive to manufacture emergencies. Guides who work on commission or who are employed by companies that participate in rescue kickback schemes have every incentive.
Understand altitude sickness symptoms before your trek. A headache at four thousand metres is normal. A headache combined with confusion, loss of coordination, and persistent vomiting is not. If your guide recommends evacuation, ask questions, what are my symptoms, have we tried descending on foot, is this genuinely urgent. A good guide will explain their reasoning clearly and without defensiveness. A guide who becomes evasive or pressuring when questioned is a guide whose advice you should not trust.
Know your insurance policy. Some policies require pre-authorisation before evacuation. Some have specific procedures for filing claims. Some exclude evacuations that are deemed medically unnecessary after the fact. Read the fine print before you leave home, not at four thousand metres in a crisis.
And if you are evacuated, whether necessarily or unnecessarily, file your insurance claim honestly and promptly. Insurance companies that detect fraudulent claims respond by raising premiums for all trekkers or by withdrawing coverage from Nepal entirely. The long-term consequence of rescue fraud is that it makes the Himalayas less safe for everyone.
What a Good Company Does Differently
At reputable companies, the evacuation decision follows a clear protocol. The guide assesses symptoms using standardised tools, pulse oximetry, the Lake Louise Acute Mountain Sickness score, and direct observation of cognitive and physical function. If symptoms are mild, the first intervention is always descent on foot, losing even five hundred metres of altitude often resolves the problem within hours. If symptoms are moderate, the guide administers medication from the first aid kit, ibuprofen for headaches, dexamethasone for suspected cerebral edema, nifedipine for suspected pulmonary edema, while preparing to descend.
Helicopter evacuation is the last resort, not the first. It is deployed when the patient cannot walk, when symptoms are escalating despite descent and medication, or when the terrain does not allow rapid descent on foot. The guide's training, experience, and judgment are the critical variables, which is why the quality of your trekking company matters more than almost any other factor in your trip.
The helicopter is not a taxi. It is an emergency medical service operating in the most challenging aviation environment on earth. Treated with the seriousness it deserves, by guides, by companies, and by trekkers, it is one of the great achievements of Himalayan tourism: the ability to reach a hospital from the roof of the world in under two hours.
Treated as a business opportunity for profit, by anyone in the chain, it becomes something uglier. The difference is in the hands of the people you choose to trust with your safety.
Travel insurance with helicopter evacuation cover is mandatory on all our treks. See the EBC Trek or Annapurna Circuit pages for full insurance requirements.
Helicopter rescue in Nepal works, but it is not free and it is not instant. Your insurance must cover it. Your guide must be able to call it. The helicopter must be able to fly (weather stops everything above 4,000 metres). When all three align, evacuation from high altitude takes two to four hours. When they do not, you wait. This is why acclimatisation, a competent guide, and proper insurance are not optional. They are the system that keeps you alive.
We carry satellite phones and pulse oximetres on every trek. Our guides are trained in altitude emergency response.
WhatsApp:+977 9810351300
Email:[email protected]
Written by Shreejan Simkhada, CEO of The Everest Holiday and third-generation Himalayan guide. TAAN Member #1586.
Want the helicopter return option from EBC? Our EBC with Helicopter Return (10 Days) is private (your group only, no strangers), 2026 dates open, From USD $4499. WhatsApp us for tailored 2026 dates and current departures.